Assessment of the Prognostic Value of Helsinki Computer Tomography Score in Severe Traumatic Brain Injury Patients at Kenyatta National Hospital in Kenya
Schlagworte:
Helsinki computer tomography score, Traumatic brain injury, Prognostic value, Neurotrauma, Glasgow coma scoreAbstract
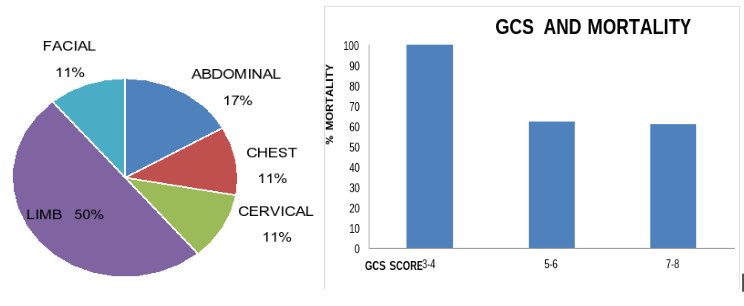
Background: Head injury is usually considered a silent epidemic, conferring high mortality and disability worldwide. In the early assessment of patients with head injury, the computer tomography is of utmost importance and millions of Computed tomography (CT) scans are conducted yearly. These CT scans contain information that can be used to determine the patient's prognosis. The Helsinki computer tomography scoring classification was developed in 2014 as a tool for determining outcomes in traumatic brain injury patients. The Helsinki computer tomography score is the most recent addition to the arsenal of outcome predictors, having outperformed previous CT scoring systems in the European and Asian subcontinents. It will be necessary to test its ability to predict outcome in patients with severe traumatic brain injury in the African subcontinent.Objectives: To assess the prognostic value of the Helsinki Computer Tomography score among patients with severe traumatic brain injury (TBI). Study Design: Prospective observational study. Setting: The Emergency Department and Critical Care Unit, Kenyatta National Hospital. Subjects: Forty-two patients with severe TBI. Results: There was a higher male preponderance at 90% (n = 38). The mean age for patients with severe TBI was 33 years old, with an overall mortality rate of 64.3%. The patients with a Helsinki CT score of 4 had a mortality rate of 33.3%, while those with a Helsinki score of 11 had a mortality rate of 100%. Patients with contusions and intracerebral hematomas had mortality rate of 80%, while in acute subdural hematoma and extradural hematoma the mortality rates were 53.8% and 44.4% respectively. Helsinki CT score was significantly associated with GOS at 6 weeks (p=0.004) and death (p=0.009). The specificity, sensitivity and accuracy for Helsinki CT score for mortality were 88.9%, 53.3% and 71% respectively; and for an unfavorable outcome, these values were 81.8%, 55.6% and 69% respectively. The odds ratio for the Helsinki CT score to predict mortality and unfavorable outcome was 9.1(95% CI 1.9-44) and 5.6(95% CI 1.2-27.4) respectively. Conclusion: Severe TBI carries a high mortality and disability in Kenya. The initial Helsinki CT score is a significant predictor of outcome.
Literaturhinweise
Masson F, Thicoipe M, Aye P, et al. Epidemiology of severe brain injuries: a prospective population based study. Journal of Trauma 2001,Sept 51: 481-489.
Guidelines for the management of severe traumatic brain injury 3rd edition. A joint project of the Brain Trauma Foundation and American Association of Neurological surgeons and Congress of Neurological Surgeons and AANS/CNS joint section on Neurotrauma and Critical Care. New York 2007.
Raj R, Siironen J, Skrifvars MB, et al. Predicting outcome in traumatic brain injury: development of a novel computerized tomography classification system (Helsinki computerized tomography score). Neurosurgery. 2014; 75(6):632-46.
MRC CRASH Trial Collaborators. Predicting outcome after traumatic brain injury: practical prognostic models based on large cohort of international patients. BMJ 2008; 336: 425-29
Marmarou A, Lu J. Butcher I, et al. Prognostic value of the Glasgow Coma Scale and pupil reactivity in traumatic brain injury assessed pre-hospital and on enrollment: an IMPACT analysis. J Neurotrauma.2007; 24: 24: 270-280.
Maas AI, Hukkelhoven CW, Marshall LF, et al. Prediction of outcome in traumatic brain injury with computed tomographic characteristics: a comparison between the computed tomographic classification and combinations of computed tomographic predictors. Neurosurgery. 2005; 57(6):1173-82.
Chesnut RM, Ghajar J, Maas AR: Guidelines for the Management and prognosis of severe traumatic brain injury part II: Early indicators of prognosis in severe traumatic brain injury. J Neurotrauma.2000; 17: 556-627.
Andriessen TM, Horn J,Franschman G, et al. Epidemiology, severity classification, and outcome of moderate and severe traumatic brain injury: A Prospective Multicenter Study. J Neurotrauma. 2011; 28(10): 2019-2031.
Teasdale G, Jennett B. Assessment of coma and severity of brain damage. Anesthesiology. 1978;49:225–6.
Perel P, Edwards P, Wentz R, et al. Systematic review of prognostic models in traumatic brain injury. BMC Med Inform Decis Mak. 2006; 6:38
Murray GD, Teasdale GM, Braakman R, et al. The European Brain Injury Consortium survey of head injuries. Acta Neurochir (Wien).1999; 141: 223-36.
Stocchetti N, Pagan F, Calappi E, et al. Inaccurate early assessment of neurological severity in head injury. J Neurotrauma. 2004; 21: 1131-40
Quigley MR, Vidovich D, Cantella D, et al. Defining the limits of survivorship after very severe head injury. J Trauma. 1997; 42(1): 7-10.
Jeremitsky E, Omert LA, Dunham CM, et al. The impact of hyperglycemia on patients with severe brain injury. J Trauma. 2005; 58(1):47–50.
Young B, Ott L, Dempsey R, et al. Relationship between admission hyperglycemia and neurologic outcome of severely brain-injured patients. Ann Surg. 1989; 210(4):466–72.
Griesdale DE, Tremblay MH, McEwen J, et al. Glucose control and mortality in patients with severe traumatic brain injury. Neurocrit Care. 2009; 11(3):311–6.
Khajavikhan J, Vasigh A, Kokhazade T, et al. Association between Hyperglycaemia with Neurological Outcomes Following Severe Head Trauma. J Clin Diagn Res. 2016; 10(4):PC11–PC13.
Chestnut RM, Marshall SB, Piek J, et al. Early and late systemic hypotension as a frequent and fundamental source of cerebral ischemia following severe brain injury in the Traumatic Coma Data Bank. Acta Neurochir Suppl (Wien). 1993; 59: 121-125.
Barmparas, G., Liou, D. Z., Lamb, et al. Prehospital hypertension is predictive of traumatic brain injury and is associated with higher mortality. Journal of Trauma and Acute Care Surgery. 2014; 77(4), 592–598.
Sarrafzadeh AS, Peltonen EE, Kaisers U, et al. Secondary insults in severe head injury – do multiply injured patients do worse? Crit Care Med. 2001; 29: 1116-23.
Seelig JM, Becker DP, Miller JD, et al. Traumatic acute subdural hematoma. N Engl J Med. 1981;304(25):1511-1518.
Haselsberger K, Pucher R, Auer LM. Prognosis after acute subdural or epidural haemorrhage. Acta Neurochir. 1988;90(3-4):111-116.
Yao S, Song J, Li S, et al. Helsinki computerized tomography scoring system can independently predict long-term outcome in traumatic brain injury, World Neurosurgery 2017 ;101: 528-53
Downloads
Veröffentlicht
Zitationsvorschlag
Ausgabe
Rubrik
Lizenz
Copyright (c) 2023 East African Journal of Neurological Sciences

Dieses Werk steht unter der Lizenz Creative Commons Namensnennung - Nicht-kommerziell - Keine Bearbeitungen 4.0 International.